Intramedullary nailing is a surgical procedure used to treat fractures of long bones, such as the femur, tibia, or humerus, by stabilizing the broken bone with a metal rod inserted into the medullary canal, the central cavity of the bone. During the procedure, the surgeon makes a small incision near the fracture site, realigns the broken bone fragments, and then inserts the nail through the marrow canal, securing it with screws at both ends to hold the bone in place while it heals. This method promotes proper alignment, reduces the risk of malunion or nonunion, and allows for early weight-bearing and faster recovery compared to other fixation techniques. Intramedullary nailing is widely regarded as a gold standard for treating complex or unstable long bone fractures due to its biomechanical advantages and minimal soft tissue disruption.
| Characteristics | Values |
|---|---|
| Definition | A surgical procedure to stabilize and align fractured long bones using a metal rod inserted into the medullary canal of the bone. |
| Purpose | Treat fractures of the femur, tibia, or humerus; promote proper healing and restore function. |
| Type of Procedure | Invasive orthopedic surgery. |
| Anesthesia | General or spinal anesthesia. |
| Duration | 1-2 hours (varies based on fracture complexity). |
| Implant Material | Titanium or stainless steel rod (intramedullary nail). |
| Fixation Method | Locked or unlocked nails with screws at both ends for stability. |
| Recovery Time | 3-6 months for full recovery; partial weight-bearing starts after 6-12 weeks. |
| Advantages | Minimal soft tissue disruption, better alignment, reduced risk of malunion. |
| Complications | Infection, malalignment, hardware failure, nerve or blood vessel injury. |
| Post-Surgery Care | Physical therapy, regular follow-ups, and weight-bearing restrictions. |
| Success Rate | High (90-95% successful union of fractures). |
| Alternative Procedures | External fixation, plating, or casting (depending on fracture type). |
| Patient Suitability | Adults and adolescents with long bone fractures; not ideal for children with open growth plates. |
| Cost | Varies by region and hospital, typically $15,000-$30,000 (U.S.). |
| Latest Advances | Biodegradable nails, minimally invasive techniques, and improved locking systems. |
Explore related products






What You'll Learn
![]()
Indications for Intramedullary Nailing
Intramedullary nailing is a surgical procedure primarily used to stabilize and align fractured long bones, such as the femur, tibia, and humerus. The procedure involves inserting a metal rod into the medullary canal of the bone, which provides structural support and promotes proper healing. Understanding when this technique is most appropriate is crucial for optimal patient outcomes.
One of the primary indications for intramedullary nailing is the treatment of diaphyseal fractures of long bones, particularly in the femur and tibia. These fractures, which occur in the shaft of the bone, often result from high-energy trauma, such as car accidents or falls from significant heights. Intramedullary nailing is favored in these cases because it allows for load-sharing, where the nail and the bone work together to bear weight, reducing the risk of implant failure. For instance, in femoral shaft fractures, the use of an intramedullary nail has been shown to provide better alignment and faster return to function compared to other methods like plating.
Another key indication is open fractures, where the broken bone pierces the skin. Intramedullary nailing is often preferred in these situations because it minimizes soft tissue disruption, reducing the risk of infection. The procedure is typically performed within 6–8 hours of injury to prevent complications. For example, in Gustilo-Anderson Grade II or III open tibia fractures, intramedullary nailing is the gold standard due to its ability to stabilize the fracture while preserving blood supply to the bone and surrounding tissues.
Pathological fractures in patients with weakened bones, such as those with osteoporosis or metastatic bone disease, are also candidates for intramedullary nailing. The procedure provides robust fixation, which is essential when the bone quality is compromised. For instance, in patients with femoral fractures secondary to metastatic cancer, intramedullary nailing can offer immediate pain relief and improved mobility, enhancing quality of life. However, careful patient selection is critical, as those with severe bone loss may require additional augmentation techniques, such as bone cement or locking screws.
Lastly, intramedullary nailing is indicated for fractures in younger, active patients who require early weight-bearing and rapid return to normal activities. The procedure’s ability to provide stable fixation allows patients to begin rehabilitation sooner, which is particularly beneficial for athletes or individuals with physically demanding jobs. For example, a 30-year-old marathon runner with a tibial shaft fracture would likely benefit from intramedullary nailing due to its high success rate and minimal impact on long-term bone function.
In summary, intramedullary nailing is a versatile procedure with specific indications that maximize its benefits. Whether treating high-energy trauma, open fractures, pathological fractures, or injuries in active individuals, this technique offers unique advantages in terms of stability, healing, and functional recovery. Proper patient selection and timing are essential to ensure the best possible outcomes.
Understanding the Black Line on Your Nail: Causes and Concerns
You may want to see also
Explore related products






![]()
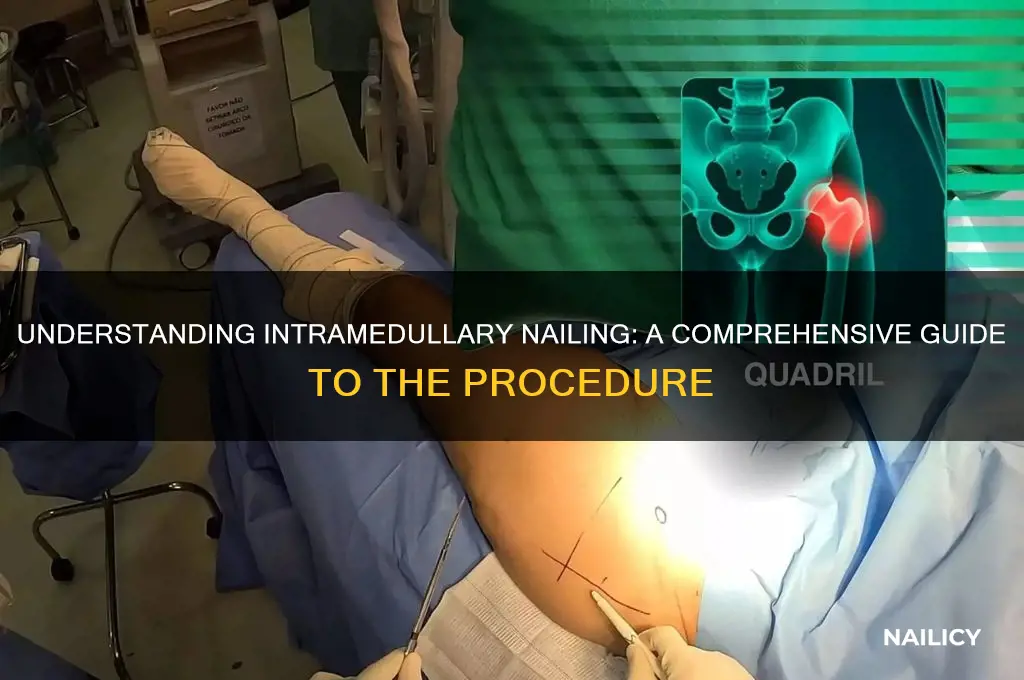
Surgical Techniques and Approaches
Intramedullary nailing is a surgical procedure primarily used to stabilize and align fractured long bones, such as the femur or tibia. The technique involves inserting a metal rod, known as an intramedullary nail, into the medullary canal of the bone, which is then secured with interlocking screws to maintain proper alignment during healing. This method has become a gold standard for treating complex or unstable fractures due to its ability to provide robust mechanical support while minimizing soft tissue disruption.
The procedure begins with careful preoperative planning, often involving CT scans or X-rays to assess the fracture pattern and determine nail length and positioning. The patient is typically placed in a supine position for femoral nailing or prone for tibial nailing, with the affected limb secured to a traction table to facilitate alignment. A small incision is made over the proximal or distal end of the bone, depending on the surgeon’s preference and fracture location. For femoral fractures, the piriformis fossa or greater trochanter is commonly used as the entry point, while tibial nails are often inserted through the tibial tuberosity.
Once the entry point is established, a guide wire is inserted into the medullary canal to guide the reaming process, which enlarges the canal to accommodate the nail. Reaming must be performed with precision to avoid thermal necrosis or further bone damage. The intramedullary nail is then inserted over the guide wire and advanced into the canal. Locking screws are placed proximally and distally to secure the nail and ensure fracture stability. Fluoroscopy is used throughout the procedure to confirm proper placement and alignment.
A critical aspect of this technique is the choice between reamed and unreamed nailing. Reamed nailing involves expanding the medullary canal to achieve a tight fit, which enhances stability but carries a higher risk of fat embolism or bone necrosis due to increased intramedullary pressure. Unreamed nailing, on the other hand, preserves the blood supply within the canal but may result in less rigid fixation, making it more suitable for osteoporotic or open fractures. The decision between these approaches depends on factors such as patient age, bone quality, and fracture complexity.
Postoperative care is essential to ensure successful outcomes. Weight-bearing restrictions are typically imposed for 8–12 weeks, depending on fracture healing. Physical therapy is initiated early to restore mobility and strength. Complications, such as malalignment, infection, or hardware failure, are rare but require prompt intervention. For instance, malalignment can lead to nonunion or malunion, necessitating revision surgery. Infection risk is minimized through strict aseptic techniques and prophylactic antibiotics, often administered within 30–60 minutes preoperatively, such as a single dose of 2 grams of cefazolin for most patients.
In conclusion, intramedullary nailing is a highly effective technique for treating long bone fractures, with surgical approaches tailored to individual patient and fracture characteristics. Precision in reaming, nail placement, and screw fixation is paramount, as is the choice between reamed and unreamed techniques. With proper execution and postoperative management, this procedure offers excellent functional outcomes and a high rate of fracture union, making it a cornerstone of modern orthopedic surgery.
Effective Remedies for Treating Painful Blood Clots Under Fingernails
You may want to see also
Explore related products






![]()
Types of Nails and Instruments
Intramedullary nailing relies on specialized nails and instruments to stabilize fractured long bones effectively. The choice of nail depends on the bone’s anatomy, fracture type, and patient factors. Nails are typically made of titanium or stainless steel, designed to withstand axial and rotational forces while promoting bone healing. They vary in length, diameter, and shape, with options like straight, curved, or telescoping designs to accommodate different bone geometries. For instance, femoral nails often feature a curved profile to match the natural bow of the femur, while tibial nails may include locking mechanisms for enhanced stability.
Instruments play a critical role in ensuring precise nail placement and fixation. A reamer is used to prepare the medullary canal, removing debris and creating space for the nail. This step is crucial to prevent thermal necrosis or bone damage, as reaming generates heat that can harm surrounding tissue. Surgeons must carefully select reamer size to avoid over-reaming, which can weaken the bone. Following reaming, a targeting device guides the nail’s insertion, ensuring alignment with the canal’s axis. Misalignment can lead to malunion or hardware failure, underscoring the importance of accurate instrumentation.
Locking screws are another essential component, securing the nail to the bone at both ends. These screws can be static or dynamic, with dynamic screws allowing controlled micromotion to stimulate bone healing. The number and placement of screws depend on the fracture pattern and bone quality. For example, in osteoporotic patients, shorter screws or alternative fixation methods may be preferred to minimize the risk of bone compromise. Advances in technology have introduced biodegradable screws, reducing the need for hardware removal in some cases.
Specialized nails cater to specific clinical scenarios. In pediatric patients, flexible nails are often used to accommodate growth plates and reduce the risk of growth disturbances. These nails are thinner and more pliable, allowing for bone remodeling as the child grows. For complex fractures or revision surgeries, modular nails with interchangeable components offer versatility in addressing unique anatomical challenges. Additionally, nails with antibiotic-coated surfaces are available for open fractures or high-infection-risk cases, providing localized prophylaxis during healing.
Practical considerations include patient positioning and imaging techniques. Fluoroscopy is commonly used to visualize nail placement in real-time, ensuring accuracy during insertion. Surgeons must balance radiation exposure with the need for precise alignment, often using pulse mode to reduce dose. Postoperatively, weight-bearing restrictions and physical therapy protocols vary based on the nail type and fracture stability. For instance, patients with interlocking nails may progress to partial weight-bearing sooner than those with non-locking constructs. Understanding these nuances ensures optimal outcomes and minimizes complications.
Mastering Domeless Nail Heating: A Step-by-Step Guide for Perfect Results
You may want to see also
Explore related products






![]()
Postoperative Care and Recovery
Immediate postoperative care following an intramedullary nailing procedure is critical to ensure proper healing and minimize complications. Patients are typically monitored in a recovery room for several hours, where vital signs are closely observed. Pain management is a priority, with opioids or non-steroidal anti-inflammatory drugs (NSAIDs) administered as needed, often through patient-controlled analgesia (PCA) pumps. Early mobilization is encouraged, starting with ankle pumps and gentle leg raises to prevent blood clots and improve circulation. Physical therapists may assist with initial exercises, ensuring the patient understands the importance of movement without compromising the surgical site.
Once discharged, patients must adhere to a structured home recovery plan. Weight-bearing restrictions are common, with partial or non-weight-bearing guidelines depending on the fracture severity and surgeon’s recommendation. Crutches or walkers are essential tools during this phase. Wound care is another critical aspect; the incision site should be kept clean and dry, with dressings changed as instructed. Signs of infection, such as redness, swelling, or discharge, require immediate medical attention. Follow-up appointments are scheduled to monitor healing progress, typically at 2, 6, and 12 weeks post-surgery, with X-rays taken to assess nail alignment and bone union.
Rehabilitation plays a pivotal role in restoring function and strength. Physical therapy begins within the first week, focusing on range-of-motion exercises for the hip, knee, and ankle. As healing progresses, weight-bearing activities are gradually reintroduced, followed by strengthening exercises targeting the quadriceps, hamstrings, and core muscles. Patients should avoid high-impact activities like running or jumping for at least 3–6 months. Swimming or stationary cycling are excellent low-impact alternatives to maintain cardiovascular fitness without straining the surgical site.
Long-term recovery involves patience and adherence to medical advice. Full healing of the femur or tibia can take 6–12 months, depending on the patient’s age, overall health, and fracture complexity. Older adults or those with comorbidities may experience slower recovery times and require additional support. Nutritional support, including adequate calcium and vitamin D intake, aids bone healing. Smoking cessation is strongly recommended, as it impairs blood flow and delays recovery. Regular communication with the healthcare team ensures any concerns are addressed promptly, fostering a smoother return to daily activities.
Mastering Block Flooring: Expert Tips for a Flawless Installation
You may want to see also
Explore related products



$249.71 $339.99



![]()
Potential Complications and Risks
Intramedullary nailing, while a highly effective procedure for stabilizing long bone fractures, carries inherent risks that demand careful consideration. One of the most immediate concerns is infection, which can occur at the surgical site or spread systemically. The risk is heightened in patients with compromised immune systems, diabetes, or those who smoke. Prophylactic antibiotics, typically administered within 30 minutes before incision, are standard practice to mitigate this risk. However, even with these measures, infection rates can range from 1% to 5%, necessitating vigilant postoperative monitoring and prompt treatment if symptoms like fever, redness, or drainage appear.
Another significant complication is malalignment or malunion, where the fractured bone heals in an improper position. This often results from inadequate reduction during surgery or improper nail placement. For instance, a varus or valgus deformity in a femoral fracture can lead to chronic pain and functional impairment. To minimize this risk, surgeons rely on intraoperative imaging, such as fluoroscopy, to ensure precise alignment. Postoperative rehabilitation, including weight-bearing restrictions and physical therapy, is equally critical to support proper healing.
Hardware-related issues are also a notable concern. The intramedullary nail or locking screws can break, migrate, or cause irritation to surrounding tissues. For example, a broken screw in a tibial nailing procedure may require revision surgery, prolonging recovery and increasing costs. Patients with osteoporosis or those subjected to high-impact activities are at greater risk. Regular follow-up imaging is essential to detect hardware failure early, and surgeons often recommend activity modifications to reduce mechanical stress on the implant.
Lastly, thromboembolic events, such as deep vein thrombosis (DVT) or pulmonary embolism (PE), pose a serious threat, particularly in lower extremity fractures. Immobilization, surgical trauma, and hypercoagulability contribute to this risk. Prophylactic measures, including low-molecular-weight heparin (e.g., enoxaparin 40 mg daily) and early ambulation, are routinely employed. Patients with a history of thrombosis or those undergoing prolonged procedures may require more aggressive anticoagulation protocols, balanced against the risk of bleeding complications.
In summary, while intramedullary nailing is a cornerstone of fracture management, its complications require proactive management. From infection control to hardware monitoring and thromboprophylaxis, a multidisciplinary approach is essential to optimize outcomes and minimize risks. Patients and providers alike must remain vigilant, as early detection and intervention are key to addressing these challenges effectively.
Master Your Audition: Proven Tips to Stand Out and Succeed
You may want to see also
Frequently asked questions
Intramedullary nailing is a surgical procedure used to stabilize and repair fractured long bones, such as the femur or tibia. It involves inserting a metal rod (nail) into the medullary canal of the bone to hold the fractured pieces together while they heal.
The procedure is performed under general anesthesia. A small incision is made near the broken bone, and a guide wire is inserted into the medullary canal. The nail is then passed over the guide wire and locked into place with screws above and below the fracture site to ensure stability.
Intramedullary nailing provides better alignment and stability for long bone fractures, reduces the risk of malunion, and allows for earlier weight-bearing and mobility. It also minimizes soft tissue disruption compared to other methods like plating.
Recovery time varies depending on the severity of the fracture and the patient’s overall health. Most patients can begin partial weight-bearing within a few weeks and return to normal activities within 3 to 6 months, though full healing may take longer.
Potential risks include infection, nerve or blood vessel damage, malalignment of the nail, or hardware failure. In some cases, the nail may need to be removed after the bone has healed, especially if it causes discomfort.