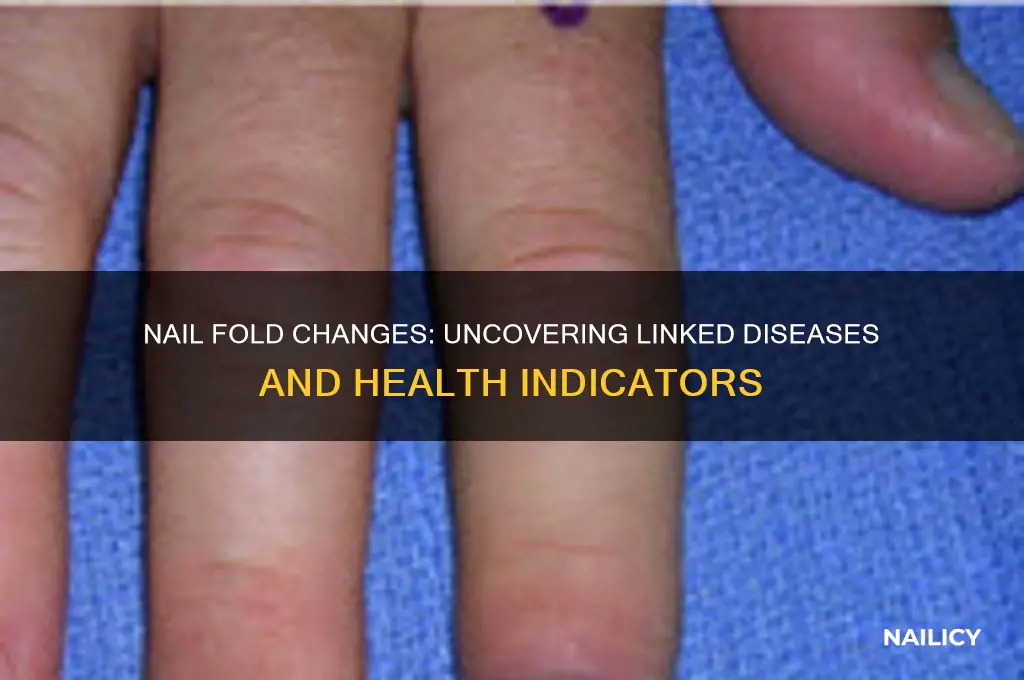
Nail fold changes, often observed during a capillaroscopy, can be indicative of various underlying diseases, particularly those affecting the connective tissues and autoimmune systems. Conditions such as systemic sclerosis (scleroderma), lupus, dermatomyositis, and rheumatoid arthritis are commonly associated with alterations in the nail fold, including capillary dilation, hemorrhage, or loss of capillaries. Additionally, infections, nutritional deficiencies, and certain medications can also manifest as nail fold abnormalities. Recognizing these changes is crucial for early diagnosis and management of the associated diseases, as they often reflect systemic involvement and disease progression.
Explore related products






What You'll Learn
- Systemic Lupus Erythematosus (SLE): Associated with nail fold capillary changes, a key diagnostic feature in lupus patients
- Scleroderma: Causes nail fold fibrosis, capillary loss, and digital ulcers, reflecting systemic vascular involvement
- Psoriasis: Linked to pitting, onycholysis, and oil drop discoloration in nail folds
- Lichen Planus: Presents with pterygium, longitudinal ridging, and nail fold inflammation
- Infectious Causes: Fungal (onychomycosis) or bacterial infections can induce redness, swelling, and nail fold damage
![]()
Systemic Lupus Erythematosus (SLE): Associated with nail fold capillary changes, a key diagnostic feature in lupus patients
Nail fold capillary changes are a subtle yet significant marker in the diagnosis of Systemic Lupus Erythematosus (SLE), a chronic autoimmune disease. These changes, observed under a dermatoscope or capillaroscope, reveal dilated, tortuous, or disorganized capillaries in the nail fold area. Such alterations are not merely cosmetic; they reflect the underlying microvascular damage caused by the inflammatory processes in SLE. For clinicians, recognizing these changes is crucial, as they can serve as an early indicator of the disease’s activity and severity, particularly in patients with cutaneous involvement.
To assess nail fold capillary changes in SLE patients, dermatologists and rheumatologists often use videocapillaroscopy, a non-invasive technique that magnifies the nail fold area up to 200 times. This method allows for detailed examination of capillary density, morphology, and architecture. Studies have shown that SLE patients frequently exhibit a "capillary dropout" pattern, where the number of capillaries per millimeter is significantly reduced compared to healthy individuals. Additionally, the presence of microhemorrhages or avascular areas further supports the diagnosis. These findings are particularly valuable in differentiating SLE from other connective tissue diseases, such as scleroderma, where nail fold changes manifest differently.
From a practical standpoint, monitoring nail fold capillary changes can guide treatment decisions in SLE management. For instance, patients with severe capillary abnormalities may require more aggressive immunosuppressive therapy to prevent further vascular damage. Conversely, improvement in capillary architecture following treatment can serve as a positive prognostic indicator. Patients should be educated about the importance of regular nail fold examinations, especially during disease flares, to ensure timely intervention. Simple self-care tips, such as avoiding trauma to the nail area and maintaining good hand hygiene, can also help preserve capillary health.
Comparatively, while nail fold changes are a hallmark of SLE, they are not exclusive to this condition. Diseases like systemic sclerosis, dermatomyositis, and mixed connective tissue disease also present with similar capillary abnormalities. However, the specific patterns observed in SLE—such as the combination of capillary dropout and microhemorrhages—help distinguish it from other disorders. This underscores the need for a comprehensive evaluation, including clinical history, serological markers, and imaging studies, to confirm the diagnosis. By integrating nail fold capillary analysis into routine assessments, healthcare providers can enhance the accuracy and efficiency of SLE diagnosis and management.
In conclusion, nail fold capillary changes are a key diagnostic feature in SLE, offering valuable insights into the disease’s microvascular pathology. Their assessment, through techniques like videocapillaroscopy, provides both diagnostic and prognostic information, aiding in tailored treatment strategies. While these changes are not unique to SLE, their specific patterns and clinical context make them a powerful tool in the rheumatologist’s arsenal. For patients, understanding the significance of these changes can foster better engagement in their care, ultimately improving outcomes in this complex autoimmune disease.
Should You Fill Nail Holes in Shiplap? A Complete Guide
You may want to see also
Explore related products






![]()
Scleroderma: Causes nail fold fibrosis, capillary loss, and digital ulcers, reflecting systemic vascular involvement
Nail fold changes can serve as early indicators of systemic diseases, and one such condition is scleroderma, a chronic autoimmune disorder characterized by skin thickening and fibrosis. Among its hallmark manifestations are nail fold fibrosis, capillary loss, and digital ulcers, which collectively reflect the disease’s profound vascular involvement. These changes are not merely cosmetic; they signal underlying microvascular damage and systemic inflammation, making them critical for early diagnosis and intervention.
Analyzing the nail fold in scleroderma reveals a distinctive pattern. Fibrosis of the nail fold, often visible as tightening and tethering of the skin, is a direct result of excessive collagen deposition. This process is driven by dysregulated fibroblast activity, a core feature of scleroderma pathophysiology. Concurrently, capillary loss occurs due to endothelial cell dysfunction and obliterative vasculopathy, leading to reduced blood flow in the nail bed. Clinicians often use nail fold capillaroscopy to assess disease severity, as the extent of capillary dropout correlates with systemic organ involvement, particularly in the lungs and kidneys.
Digital ulcers, another complication of scleroderma-related nail fold changes, arise from ischemia and repetitive microtrauma. These painful lesions are a significant source of morbidity, often requiring multidisciplinary management. Treatment strategies include vasodilators like calcium channel blockers (e.g., nifedipine 30–60 mg/day) to improve blood flow, topical nitrates for localized ischemia, and phosphodiesterase-5 inhibitors (e.g., sildenafil 20–40 mg tid) to enhance vascular perfusion. Patients are also advised to avoid exposure to cold temperatures, wear protective gloves, and maintain meticulous hand hygiene to prevent infection.
Comparatively, while other diseases like systemic lupus erythematosus (SLE) or dermatomyositis may also present with nail fold changes, scleroderma’s triad of fibrosis, capillary loss, and digital ulcers is unique. This specificity underscores the importance of recognizing these signs as red flags for systemic vascular involvement. Early referral to a rheumatologist is crucial, as timely initiation of disease-modifying therapies, such as mycophenolate mofetil (1–3 g/day) or methotrexate (10–25 mg/week), can slow disease progression and preserve function.
In conclusion, nail fold changes in scleroderma are more than superficial markers; they are windows into the disease’s systemic vascular pathology. By understanding the mechanisms behind fibrosis, capillary loss, and digital ulcers, healthcare providers can adopt a proactive approach to management. Patients, too, play a vital role in monitoring their symptoms and adhering to treatment regimens, ensuring that these subtle yet significant signs are not overlooked.
Does Losing a Nail Hurt? Understanding the Pain and Healing Process
You may want to see also
Explore related products






![]()
Psoriasis: Linked to pitting, onycholysis, and oil drop discoloration in nail folds
Nail changes are often subtle yet telling signs of underlying health conditions, and psoriasis stands out as a prime example. This chronic autoimmune disorder, affecting approximately 2-3% of the global population, frequently manifests in the nails, offering clues to its presence and severity. Among the most characteristic nail alterations associated with psoriasis are pitting, onycholysis, and oil drop discoloration. Recognizing these changes is crucial for early diagnosis and targeted treatment, as they can significantly impact a patient’s quality of life.
Pitting, the most common nail manifestation in psoriasis, appears as small depressions or holes on the nail surface. These pits result from the abnormal growth of keratinocytes in the nail matrix, a hallmark of psoriatic inflammation. Studies indicate that up to 50% of psoriasis patients exhibit pitting, often correlating with the severity of skin involvement. For instance, individuals with moderate to severe plaque psoriasis are more likely to develop pronounced pitting. Clinicians often use the number and depth of pits as a diagnostic marker, though it’s essential to differentiate them from similar findings in conditions like eczema or alopecia areata.
Onycholysis, another frequent nail change in psoriasis, involves the detachment of the nail plate from the nail bed. This separation can lead to a white or yellowish discoloration and, if left untreated, may allow fungi or bacteria to infiltrate the gap, causing secondary infections. Onycholysis is particularly problematic because it can mimic other disorders, such as fungal infections or thyroid disease. Patients often report discomfort or pain, especially if the nail becomes snagged or torn. Treatment strategies typically include topical corticosteroids or calcineurin inhibitors to reduce inflammation, alongside antifungal agents if infection is present.
Oil drop discoloration, though less common than pitting or onycholysis, is highly specific to psoriasis. This unique finding appears as small, yellow-brown spots resembling oil drops beneath the nail plate. It occurs due to the accumulation of psoriatic cells and hemosiderin deposits in the nail bed. While oil drop discoloration is not painful, it can be a source of cosmetic concern for patients. Dermatologists often use dermoscopy to confirm this feature, as it is rarely visible to the naked eye in early stages. Recognizing oil drop discoloration is invaluable, as it strengthens the case for a psoriatic diagnosis, particularly in patients with minimal skin or joint involvement.
In managing psoriatic nail changes, a multifaceted approach is key. Topical treatments, such as high-potency corticosteroids (e.g., clobetasol 0.05% applied once daily) or vitamin D analogs (e.g., calcipotriene), are often first-line therapies. For severe cases, systemic medications like methotrexate, acitretin, or biologics (e.g., ustekinumab, secukinumab) may be necessary. Patients should also be advised to keep nails trimmed and avoid trauma, as even minor injuries can exacerbate symptoms. Regular monitoring by a dermatologist is essential, as nail psoriasis can be a predictor of joint involvement (psoriatic arthritis) in up to 10% of cases. By addressing these nail changes promptly, healthcare providers can improve both the physical and emotional well-being of patients living with psoriasis.
Mastering Elegant Touch Nail Glue: A Step-by-Step Application Guide
You may want to see also
Explore related products






![]()
Lichen Planus: Presents with pterygium, longitudinal ridging, and nail fold inflammation
Nail fold changes can be indicative of various underlying health conditions, and one such condition is lichen planus, a chronic inflammatory disorder affecting the skin, mucous membranes, and nails. This disease presents a unique set of symptoms, including pterygium, longitudinal ridging, and nail fold inflammation, which can significantly impact a person's quality of life.
Understanding the Symptoms
Pterygium, a hallmark of lichen planus, refers to the abnormal growth of fibrous tissue that can cause the nail to become adhered to the underlying skin, leading to a raised, triangular-shaped fold. This condition can affect one or more nails and may result in nail thickening, distortion, and even loss. Longitudinal ridging, another characteristic feature, appears as vertical lines or grooves running from the base to the tip of the nail. These ridges can be subtle or pronounced, often accompanied by nail thinning and fragility. The inflammation of the nail fold, known as paronychia, causes redness, swelling, and tenderness around the nail's base, potentially leading to pain and discomfort.
Diagnosis and Treatment Approach
Diagnosing lichen planus involves a comprehensive evaluation by a dermatologist. A detailed medical history, physical examination, and, in some cases, a nail biopsy are essential steps. Treatment strategies aim to manage symptoms and prevent complications. Topical corticosteroids are often the first-line therapy, applied directly to the affected nails and surrounding skin to reduce inflammation and improve appearance. For more severe cases, oral medications such as acitretin or immunosuppressants might be prescribed, but these require careful monitoring due to potential side effects.
Practical Management and Self-Care
Patients with lichen planus-related nail changes can benefit from specific self-care practices. Keeping nails trimmed and avoiding aggressive manicures can prevent trauma and further damage. Moisturizing the nail folds regularly with emollient-rich creams helps maintain skin integrity and reduce inflammation. Additionally, protecting hands and nails from harsh chemicals and wearing gloves during household chores can minimize irritation. It is crucial to monitor any changes in nail appearance and seek medical advice promptly, as early intervention can significantly improve treatment outcomes.
Long-term Outlook and Patient Education
Lichen planus is a chronic condition, and nail changes may persist or recur over time. Patient education plays a vital role in management. Understanding the disease process, recognizing triggers, and adhering to treatment plans are essential for long-term care. Support groups and online resources can provide valuable insights and coping strategies for individuals dealing with the cosmetic and functional impacts of this disease. Regular follow-ups with healthcare providers ensure ongoing assessment and adjustment of treatment modalities, ultimately aiming for symptom control and improved patient well-being.
Elegant French Tip Nails: Mastering Shellac Application at Home
You may want to see also
Explore related products





![]()
Infectious Causes: Fungal (onychomycosis) or bacterial infections can induce redness, swelling, and nail fold damage
Nail fold changes often signal underlying health issues, and infectious causes—particularly fungal and bacterial infections—are among the most common culprits. These infections can lead to visible symptoms such as redness, swelling, and damage to the nail fold, the skin that frames the nail plate. Recognizing these signs early is crucial, as untreated infections can progress to more severe complications, including permanent nail deformity or systemic spread in immunocompromised individuals.
Fungal infections, specifically onychomycosis, are a leading cause of nail fold changes. Onychomycosis is primarily caused by dermatophytes, though yeasts and molds can also be responsible. The infection often begins as a small yellow or white spot under the nail tip, gradually spreading deeper, causing thickening, discoloration, and crumbling of the nail. The nail fold may become inflamed, tender, and swollen as the infection progresses. Treatment typically involves topical antifungal agents like efinaconazole or tavaborole for mild cases, while oral medications such as terbinafine (250 mg daily for 6–12 weeks) are prescribed for more severe or stubborn infections. Maintaining proper foot hygiene, wearing breathable footwear, and avoiding walking barefoot in public areas can reduce the risk of recurrence.
Bacterial infections, though less common than fungal ones, can also affect the nail fold, particularly in cases of paronychia. Acute paronychia often results from bacterial pathogens like *Staphylococcus aureus* entering the skin through cuts or breaks in the nail fold. Symptoms include redness, swelling, warmth, and pus formation. Treatment involves warm soaks to encourage drainage and, in severe cases, oral antibiotics such as cephalexin (500 mg every 6 hours for 7–10 days) or clindamycin for those allergic to penicillin. Chronic paronychia, often associated with Candida species in addition to bacteria, requires addressing underlying causes like frequent hand exposure to water or irritants. Protective gloves and topical antifungal/steroid combinations (e.g., betamethasone with clotrimazole) are recommended for management.
Comparing fungal and bacterial infections highlights the importance of accurate diagnosis. While both can cause redness and swelling, fungal infections typically present with gradual nail thickening and discoloration, whereas bacterial infections often manifest acutely with pus and rapid onset of pain. Misdiagnosis can lead to ineffective treatment, such as using antifungals for a bacterial infection or vice versa. A potassium hydroxide (KOH) preparation or nail culture can confirm fungal etiology, while bacterial cultures guide antibiotic selection. Early intervention not only alleviates discomfort but also prevents long-term cosmetic and functional damage to the nail unit.
In summary, infectious causes of nail fold changes demand prompt attention and targeted therapy. Fungal infections like onychomycosis require systemic or topical antifungals, while bacterial paronychia often necessitates antibiotics and local care. Understanding the distinct clinical features and treatment approaches for these infections ensures effective management and minimizes complications. Regular monitoring and preventive measures, such as keeping nails dry and avoiding trauma, are essential to maintaining nail health and preventing recurrent infections.
Mastering the Dream Nail: A Comprehensive Guide to Full Awakening
You may want to see also
Frequently asked questions
Nail fold changes refer to abnormalities in the skin around the nails, such as swelling, redness, or capillary changes. They are significant because they can indicate underlying systemic diseases, particularly autoimmune or vascular conditions.
Nail fold changes are commonly associated with systemic lupus erythematosus (SLE), scleroderma, and dermatomyositis. These changes often include capillary dilation, hemorrhages, or sclerotic skin.
Yes, nail fold changes such as clubbing (enlarged fingertips with curved nails) can be associated with cardiovascular diseases like congenital heart defects or chronic ischemic heart disease.
Yes, infections like paronychia (nail fold inflammation) or systemic fungal infections can cause nail fold changes. Additionally, conditions like HIV may present with nail fold abnormalities due to immune compromise.