Nail psoriasis is a condition that affects the nails, causing changes in their appearance and texture, and understanding its origin is crucial for effective management. The question of whether nail psoriasis starts at the nail bed is significant, as it can influence treatment approaches and patient outcomes. Research suggests that nail psoriasis often begins in the nail matrix, the area responsible for nail growth, but the nail bed, which lies beneath the nail plate, can also be involved in the disease process. This involvement may lead to symptoms such as pitting, ridging, discoloration, and even separation of the nail from the nail bed. Recognizing the role of the nail bed in the development of nail psoriasis is essential for dermatologists and patients alike, as it highlights the need for targeted therapies that address both the matrix and the bed to achieve comprehensive symptom relief.
| Characteristics | Values |
|---|---|
| Origin of Nail Psoriasis | Nail psoriasis can start at the nail matrix (the area under the cuticle where the nail is formed) rather than the nail bed. However, changes in the nail bed can also occur as a result of psoriasis. |
| Initial Symptoms | Early signs may include pitting (small dents in the nail), discoloration (yellow-brown spots), or thickening of the nail. |
| Progression | Over time, the nail may become loose, crumble, or separate from the nail bed (onycholysis). |
| Affected Areas | Both fingernails and toenails can be affected, with toenails often more severely impacted. |
| Underlying Cause | Psoriasis, an autoimmune condition, causes rapid skin cell growth, leading to nail changes when it affects the nail matrix or bed. |
| Diagnosis | Diagnosed through physical examination, medical history, and sometimes nail biopsy to rule out other conditions. |
| Treatment | Treatments include topical medications, corticosteroids, vitamin D analogs, phototherapy, and systemic medications targeting psoriasis. |
| Prevalence | Nail psoriasis affects approximately 50% of individuals with psoriasis and up to 78% of those with psoriatic arthritis. |
| Complications | Secondary infections, pain, and functional impairment can occur due to severe nail changes. |
| Prognosis | Management focuses on controlling symptoms, as there is no cure. Early treatment can improve nail appearance and function. |
Explore related products






What You'll Learn
- Nail Psoriasis Origins: Does it begin at the nail bed or elsewhere
- Symptoms at Nail Bed: Early signs of psoriasis in the nail bed
- Nail Bed Anatomy: Role of the nail bed in psoriasis development
- Psoriasis Progression: How it spreads from the nail bed to the nail
- Diagnosis at Nail Bed: Identifying psoriasis starting at the nail bed
![]()
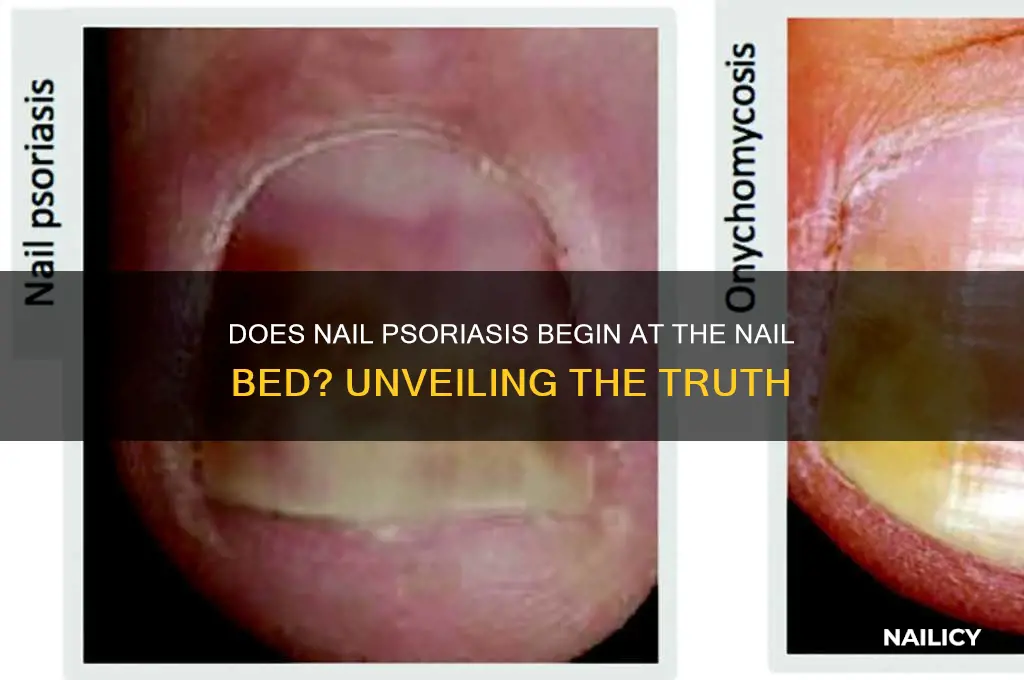
Nail Psoriasis Origins: Does it begin at the nail bed or elsewhere?
Nail psoriasis, a condition affecting up to 50% of individuals with psoriasis, often raises questions about its origin. The nail bed, a critical structure beneath the nail plate, is frequently implicated as the starting point. However, recent studies suggest that the inflammation associated with psoriasis may not always originate here. Instead, it could stem from the matrix—the area responsible for nail growth—or even systemic factors influencing the entire nail unit. Understanding this distinction is crucial, as it impacts treatment approaches, such as whether to focus on topical therapies for the nail bed or systemic medications for broader inflammation.
To determine the origin, dermatologists often examine the nail’s appearance. Pitting, a hallmark of nail psoriasis, occurs when the matrix is affected, leading to irregular nail plate formation. In contrast, onycholysis (separation of the nail from the nail bed) and subungual hyperkeratosis (thickening beneath the nail) suggest involvement of the nail bed or hyponychium. For instance, if pitting is the sole symptom, treatments like calcipotriene or tazarotene, which target the matrix, may be prioritized. However, if onycholysis is present, antifungal therapies or corticosteroids might be more effective, as they address nail bed inflammation.
A comparative analysis of treatment outcomes further highlights the importance of origin identification. Systemic medications like methotrexate or biologics (e.g., adalimumab, dosed at 40 mg every other week for adults) are often prescribed for severe cases, regardless of the origin, due to their ability to modulate systemic inflammation. However, for localized symptoms, such as mild pitting or discoloration, topical treatments like 5% fluorouracil cream applied nightly can yield results within 12–16 weeks. This tailored approach underscores the need to pinpoint whether the nail bed or matrix is primarily affected.
Practical tips for patients include monitoring nail changes closely, as early detection can improve treatment efficacy. For example, keeping nails trimmed and avoiding trauma can prevent exacerbation of symptoms. Additionally, incorporating moisturizers with urea or salicylic acid can help manage dryness and thickening. While these measures do not address the origin directly, they support overall nail health, making it easier to identify and treat the root cause. Ultimately, a nuanced understanding of nail psoriasis origins empowers both clinicians and patients to adopt more effective, personalized treatment strategies.
Easy Steps to Apply What Up Nail Stickers for Perfect Manicures
You may want to see also
Explore related products






![]()
Symptoms at Nail Bed: Early signs of psoriasis in the nail bed
Nail psoriasis often begins subtly, with changes at the nail bed that can be mistaken for minor injuries or fungal infections. One of the earliest signs is pitting, where small, pinhead-sized depressions appear on the nail surface. These pits are caused by abnormal growth at the nail matrix, the area where the nail is formed. While pitting is a hallmark of psoriasis, it’s not always present in the early stages, making it crucial to observe other symptoms. For instance, a salmon-colored patch or oil drop discoloration under the nail may emerge, resembling a drop of oil or blood beneath the surface. These changes are often overlooked but can be early indicators of psoriasis, especially when accompanied by other nail abnormalities.
Another early symptom is onycholysis, where the nail separates from the nail bed, creating a white or yellowish gap. This occurs because psoriasis disrupts the normal adhesion between the nail plate and the underlying tissue. While onycholysis can result from trauma or infection, its presence alongside other psoriasis symptoms—like thickening or crumbling of the nail—should raise suspicion. It’s important to note that these changes typically start at the free edge of the nail and progress toward the cuticle, a pattern that distinguishes psoriasis from conditions like fungal infections, which often begin at the cuticle.
For those monitoring their nails, subungual hyperkeratosis is another red flag. This condition causes thickening of the skin under the nail, leading to a raised, rough appearance. While it’s more common in advanced cases, early-stage psoriasis may present with mild thickening that feels gritty or uneven to the touch. This symptom often coincides with nail plate crumbling, where the nail becomes brittle and breaks easily. If you notice these changes, particularly in multiple nails, it’s advisable to consult a dermatologist, as early intervention can prevent further damage.
A comparative analysis of nail psoriasis versus fungal infections highlights the importance of accurate diagnosis. Fungal infections typically cause yellow-brown discoloration, thickening, and debris under the nail, often starting at the distal edge. In contrast, psoriasis-related changes are more varied, with pitting, oil spots, and onycholysis being key differentiators. While over-the-counter antifungal treatments may temporarily improve symptoms, they won’t address the underlying autoimmune cause of psoriasis. For this reason, a biopsy or dermoscopy may be necessary to confirm the diagnosis, especially in ambiguous cases.
Practically speaking, early detection relies on vigilance and regular nail examination. If you’re at higher risk—due to a family history of psoriasis or existing skin psoriasis—inspect your nails weekly for subtle changes. Keep nails trimmed and clean to minimize trauma, which can exacerbate symptoms. Avoid harsh chemicals or excessive moisture, as these can irritate the nail bed. If you suspect psoriasis, document changes with photos to track progression and share with your healthcare provider. While nail psoriasis can’t be cured, early treatment with topical steroids, vitamin D analogs, or systemic medications can manage symptoms and preserve nail health.
Easy Guide to Applying Soft Claws Nail Caps for Cats
You may want to see also
Explore related products




![]()
Nail Bed Anatomy: Role of the nail bed in psoriasis development
The nail bed, a delicate matrix of cells and tissues, serves as the foundation for nail growth and health. In the context of psoriasis, understanding its anatomy is crucial. This thin layer of skin beneath the nail plate is where keratinocytes proliferate, a process that, when accelerated, can lead to the characteristic thickening and discoloration seen in nail psoriasis. The nail bed’s proximity to the nail matrix—the area responsible for nail formation—means that any inflammation or abnormal cell turnover here can directly impact nail appearance and structure. This anatomical relationship underscores why nail psoriasis often manifests as pitting, ridging, or even separation of the nail from the bed.
Consider the nail bed as a canvas where psoriasis paints its symptoms. Unlike skin psoriasis, which often presents as plaques or scales, nail psoriasis is subtler but equally debilitating. The nail bed’s role is twofold: it nourishes the nail plate and acts as a barrier. When psoriasis disrupts this function, the nail loses its smooth texture and clarity. For instance, onycholysis—separation of the nail from the bed—occurs when psoriasis-induced inflammation weakens the bond between these layers. This process highlights how the nail bed’s integrity is pivotal in both nail health and disease progression.
To illustrate, imagine a garden where the soil (nail bed) determines the health of the plant (nail). If the soil is compromised, the plant withers. Similarly, psoriasis in the nail bed affects the nail’s growth cycle, often leading to deformities like Beau’s lines or oil spots. These symptoms arise from the nail bed’s inability to support normal keratinization due to inflammation. Clinically, this is why treatments targeting the nail bed, such as topical corticosteroids or calcineurin inhibitors, are often prescribed. These therapies aim to reduce inflammation and restore the nail bed’s function, thereby improving nail appearance.
A comparative analysis reveals that while skin psoriasis is driven by similar immune mechanisms, the nail bed’s confined space amplifies the impact of inflammation. The nail’s slow growth cycle—approximately 3-6 months for fingernails—means that damage to the nail bed takes longer to repair. This anatomical constraint necessitates early intervention. For patients, monitoring changes in the nail bed, such as redness or tenderness, can be a practical tip for detecting psoriasis early. Dermatologists often emphasize the importance of treating nail psoriasis promptly to prevent irreversible damage to the nail structure.
In conclusion, the nail bed’s role in psoriasis development is both structural and functional. Its anatomical position as the nail’s support system means that any disruption here directly translates to visible nail changes. Understanding this relationship not only aids in diagnosis but also guides treatment strategies. For those affected, recognizing the nail bed’s significance can empower proactive management, ensuring healthier nails and improved quality of life.
Sparkling Nail Art: Mastering Firework Designs for Festive Manicures
You may want to see also
Explore related products






![]()
Psoriasis Progression: How it spreads from the nail bed to the nail
Nail psoriasis often begins subtly, with changes originating in the nail matrix—the area beneath the cuticle where cells are generated. This hidden onset is why early symptoms like pitting or discoloration might go unnoticed until the condition progresses to more visible parts of the nail. Understanding this progression is key to early intervention, as the nail matrix is responsible for producing the nail plate, and damage here can lead to long-lasting deformities.
The spread from the nail bed to the nail plate occurs as the psoriasis-affected cells multiply rapidly, altering the nail’s structure. For instance, onycholysis—separation of the nail from the nail bed—develops as the disease advances, creating a gap where debris accumulates. This process is not uniform; some nails may show only mild pitting, while others develop severe thickening or crumbling. The rate of progression varies, influenced by factors like immune system activity, trauma, or infections, making each case unique.
To slow this progression, targeted treatments are essential. Topical therapies, such as corticosteroids or vitamin D analogs, can be applied directly to the nail folds and cuticle area to address inflammation at its source. For more advanced cases, systemic medications like methotrexate or biologics may be prescribed, often in doses tailored to the patient’s age, weight, and disease severity. Practical tips include keeping nails trimmed to reduce pressure on the nail bed and avoiding harsh chemicals that can exacerbate irritation.
Comparing nail psoriasis to skin psoriasis highlights the importance of early detection. While skin lesions are immediately visible, nail changes can be mistaken for fungal infections or minor injuries. A dermatologist can differentiate through examination or a biopsy, ensuring appropriate treatment. Unlike skin psoriasis, which often responds to light therapy, nail psoriasis requires more persistent management due to the nail’s slower growth cycle—typically 3–6 months for noticeable improvement.
In conclusion, the progression of nail psoriasis from the nail bed to the nail is a gradual, often insidious process that demands vigilance. By recognizing early signs and employing targeted treatments, individuals can mitigate damage and preserve nail health. This approach underscores the need for personalized care, combining medical intervention with lifestyle adjustments to manage this chronic condition effectively.
Quick Fix for Ripped Nails: Reconnect and Repair in Minutes
You may want to see also
Explore related products






![]()
Diagnosis at Nail Bed: Identifying psoriasis starting at the nail bed
Nail psoriasis often begins at the nail matrix, the area where the nail is formed, rather than the nail bed itself. However, early signs can appear in both regions, making a thorough examination crucial for accurate diagnosis. The nail bed, located beneath the nail plate, may show symptoms like discoloration, pitting, or oil drop discoloration, which are hallmark indicators of psoriasis. Recognizing these signs early can lead to timely intervention and management of the condition.
Observation and Analysis:
When inspecting the nail bed for psoriasis, look for small, pinpoint pits resembling thimble-like depressions. These pits are caused by abnormal keratinization in the nail matrix but are visible on the nail bed. Another telltale sign is onycholysis, where the nail separates from the nail bed, often accompanied by a yellowish-white discoloration. Oil drop discoloration, characterized by small, yellow-brown spots, is another key marker. These symptoms, when observed in conjunction with skin psoriasis, strongly suggest nail psoriasis. However, they can also occur in isolation, making a detailed examination essential.
Practical Steps for Identification:
To diagnose nail psoriasis starting at the nail bed, begin by examining the nail under good lighting. Use a magnifying glass or dermatoscope for a closer look. Note any changes in texture, color, or structure. Compare the affected nail to healthy nails for contrast. If pitting or onycholysis is present, document the severity and location. For oil drop discoloration, assess whether the spots are uniform or scattered. If unsure, consult a dermatologist for a biopsy or imaging to rule out fungal infections or other conditions with similar presentations.
Cautions and Considerations:
Misdiagnosis is common in nail psoriasis due to its similarity to other nail disorders like eczema, lichen planus, or fungal infections. For instance, pitting can also occur in alopecia areata, and onycholysis is seen in thyroid disorders. Always consider the patient’s medical history, especially if they have plaque psoriasis or psoriatic arthritis. Avoid relying solely on visual inspection; laboratory tests like potassium hydroxide (KOH) preparations can help exclude fungal causes. Early misdiagnosis can delay appropriate treatment, worsening the condition and impacting quality of life.
Takeaway and Management Tips:
Identifying nail psoriasis at the nail bed stage allows for targeted treatment, such as topical corticosteroids, vitamin D analogs, or systemic therapies like methotrexate or biologics for severe cases. Practical tips include keeping nails trimmed and clean to prevent secondary infections. Patients should avoid trauma to the nails, as it can exacerbate symptoms. Regular follow-ups with a dermatologist are essential to monitor progress and adjust treatment plans. While nail psoriasis is chronic, early and consistent management can significantly improve nail appearance and function.
From Wire to Fastener: The Manufacturing Process of Nails and Staples
You may want to see also
Frequently asked questions
Nail psoriasis often begins at the nail matrix (the area where the nail grows), but it can also affect the nail bed, leading to symptoms like pitting, discoloration, and thickening.
While some symptoms like pitting or ridges may appear on the nail surface, these changes typically originate from the nail matrix or bed, as psoriasis disrupts the growth process.
Yes, nail psoriasis can start at the nail bed and progress to affect the entire nail, causing symptoms like oil spots, thickening, and separation from the nail bed.